Talk:Antepartum Record
Jump to navigation
Jump to search
5/5/2009: applied CP-PCC-0048
Action Items
- for Glossary terms:
Review terms and define as if being read outside of AR profileAnne: Spell out abbreviations - is this done?Review definitions for context definitionsAnne: Use consistent tense across all terms
- for Volume I:
Anne: address "todo" labelsAnne: internationalize introAnne: Quick summary for use case at beginning of each
- for Volume II:
Tone: add data type columns to data element tablesthis likely needs further analysisTone: restructure Medical History section to use the data element as the <value>Keith/Larry/Tone: determine how to handle "not asked" for medical history (and other) elements. using negation indicatorTone: determine which elements are required and which are optional for APH&PTone: Align APL with XD-LAB?may need some additional wordingTone: Discuss and determine direction to go on APE - can we use the current PCC education structure?- Tone: Include additional psych-social coded elements in Social History (mental illness, homelessness, etc.)
Tone: Input Lab LOINC codes from spreadsheetTone: Input Education snomed codes from spreadsheet- Tone/Christine: Review and finalize snomed codes for APH&P
- Tone/Christine: Review and finalize snomed codes for APE
- Tone/Mike Jolley: Review and finalize LOINC codes for APL
Tone: move Gynelogical/Menstrual History to ROS- Tone: Finish examples for:
- Medical History
- Review of Systems
- Physical Examination
- Vital Signs
- Tone: optional coded procedures in Medical History for Gyn Surgery and Operations/Hospitalizations
Tone: add raceCode in addition to ethnicityCodeTone: Create new section for infection history/History of InfectionTone: Move Genetic Screening out of ROS and into new section. this section was moved into Family History instead- Anne: Picture for process flow
Form A&B History and Physical
TODO:
- Align PCC(CRS) Header with with CDA4CDT Header - i think it will be just the inclusion of a couple of nodes
- Add discrete data elements in tables
- Generate example xml
Spreadsheets and other files
- Fields split into appropriate sections with possible loinc codes: media:APS_Field_Mapping_Forms_A&B.xls
- Updated snomed/loinc code spreadsheet 05-14-2008: media:ACOG_Mapping_Forms_AB_20080514.xls
- Updated snomed/loinc code spreadsheet 05-28-2008: media:ACOG_Mapping_Forms_AB_20080528.xls
- Below are the translated French perinatal documents:
Technical Notes/Questions
- proposing to use CDA4CDT H&P for much of this
- need to define Gynecological History
- some LOINCs were found in last years work, but what about those fields which do not have LOINC codes? should we compose a list and submit for new codes?
- (4/18 ts from discussion with Mike Jolley) Should we consider using Snomed codes here as there may be more codes available?
- Alschuler Associates to review and provide feedback
- (4/14 ts) - Remapped the ACOG data elements to CDA4CDT elements
- (4/18 ts) I see 3 options here for the basic structure for basing this on CDA4CDT History & Physical:
- Reference all CDA4CDT H&P sections and extend where necessary - this will have circular references - (i.e. CDA4CDT Review of Systems references IHE Review of Systems)
- Reference CDA4CDT only where not found in IHE - and extend both the CDA4CDT and IHE sections where necessary
- Mix and match CDA4CDT and IHE sections where appropriate
- (4/18 ts) Is it ok to reference CDA4CDT piecemeal? (i.e. only reference sections applicable to APS)
- (5/9 ts) There are 2 sections regarding Pregnancy History on Form A
- Gravida Para Abortus (just above Menstrual History)
- This is a summary of the past pregnancies and even though it may often be extracted from the Past Pregnancy Section, it needs its own section as many emr systems and clinics may not collect detailed Past Pregnancy History
- Should add a data element here for Live Births
- Past Pregnancy History
- This is detailed information about the past pregnancies
- Should be a Required if Known section as some emr systems and/or clinics will not capture this information
- Gravida Para Abortus (just above Menstrual History)
from T-Conn 4/18/08 (ts)
- there should be 2 document specifications
- the PCC generic History and Physical template
- the APS specific History and Physical template that further constrains the generic one
- The goal of this approach is to have a PCC document that is also compliant with the CDA4CDT H&P that is currently in DSTU
- Need to be careful to avoid copyright issues
- will include Medications and Allergies - from an APS perspective this means these sections will be in both this document and the Form C document, but that's ok.
- This document needs to stand on its on and not be tied directly to the CDA4CDT - this is to facilitate an easier implementation
Clinical Questions
- (4/25 ts) Are there any additional Genetic Screen/Teratology Counseling items other than what is on Form B to be considered?
from Clinical T-Conn 5/1/08 (ts)
- Add these to the Genetic Screening/Teratology Counseling List:
- Hydrocephaly
- History of cleft Lip or palate
- Polycystic kidney disease
- PKU for infant is being considered, but since this is an antepartum (and not postpartum) record it does not really apply here
- Mike Jolley has found some Snomed codes for Forms A&B
- Be careful with Physical Education so that it is not constrained to "normal" and "abnormal" checkboxes as displayed on the form. Should allow for emr systems that do not capture data in this particular format
Form D Labs
Spreadsheets and other files
- LOINC codes provided by Clem McDonald - some questions need to be answered here. Refer to section beginning at L1. media:2008_04_UHIN_Perinatal_Record_20070801_(CCR_and_CCD_Mapping)_blinded_revision(4).xls
- Updated LOINC code spreadsheet 5/15/08 media:Form D Labs (LOINC Questions) 20080516 (Draft).xls
- Sample lab results:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Technical Notes/Questions
- using LOINC coding for this
- (4/18 ts) Please advise which specific labs sample results are needed for and I can provide.
- (4/18 ts) Mike Jolley has scheduled meeting with Intermountain folks to review LOINC codes
- (5/8 ts) My thoughts are that we can only provide a "suggested use" list of loinc codes because of the variety of methods of administration and results. There does need to be a section code specifying this is an antepartum specific lab results document though.
- (5/8 ts) After a discussion with Clem McDonald, I am thinking that a Survey Panel with an entry that can have multiple procedures should be used instead of just an entry with multiple procedures. This will allow for labs that are administered in panels.
- (5/14 ts) Mike Jolley suggests: to allow for using proprietary codes and LOINC codes to aid in the transition to a standards only coding system
Clinical Questions
From Clem McDonald 4/4:
- Presume that chlaymdyia and GC is asking for DNA testing for the presence of those organisme
- And that the rubella and varicella is asking for the antibodies not the antigens
- The triple screen is an old thing- and believe that most people now do a quad screen or better.
- Don't understand hemoglobin as an optional test since it is included in the required tests HCT/Hgb/MCV (hgb is an abbreviation for hemoglobin)
- am not sure what kind of test they are doing regarding cystic fibrosis, tay sachs familial dysautomina. Are those tests on mother or father?
- Questions about family history or tests on the fetus s?
From Tone Southerland 4/8:
- Need to discuss and understand why the lab results are split into groups to help determine appropriate way to represent the data in the CDA document.
- Should it be a collection of panels - each panel representing a group (24-28 Weeks, etc.)? This approach is needed if the same lab can be administered at multiple times in a pregnancy with results that can be interpreted differently based on that administration time frame.
- Or should they all be simple observations and let the implementers determine which group the lab belongs in based on the effectiveTime?
from Clinical T-Conn 5/1/08 (ts)
- After much discussion it was decided to not use the ACOG lab groupings, but instead to specify in the PCC framework that the lab results are to be rendered by the content consumer in date order from earliest to latest to resemble the ACOG groupings. The ACOG groupings are laid out to guide the provider on when to perform the labs - so they are generally administered from earliest to latest date by weeks gestation.
- Each lab result will have a verifier, or a signoff - if an EMR system uses a document or encounter level signoff then that provider is to also act as the signoff for the individual labs. To much degree this is up to the implementer - we just need to provide a method to implement this.
- The date to be used for the lab tests is the order or sampling date - NOT the date the result was received
- Mike Jolley is working on finalizing the LOINC codes and after review with Intermountain folks (and maybe others) will submit to the group for approval
Form E Education
Spreadsheets and other files
- currently this spreadsheet does not have any codes:
media:APS_Field_Mapping_Form_E.xls
- updated APE codes spreadsheet: media:APS_Field_Mapping_Form_E_20080519.xls
- updated APE codes spreadsheet: media:APS_Field_Mapping_Form_E_v2_20080528.xls
Technical Notes/Questions
- proposing to use Snomed coding for this.
- (4/11 ts) Keith is to write a new general education section (i think..) that APS Education can further constrain
from T-Conn 5/2/08 (ts)
- Keith has not had time to write general education section so Tone is going to look into it
- Tone mentioned that we should not use the ACOG trimester groupings and it was accepted that this is the way to go.
- Keith mentioned not to use the existing Patient Education and Consents sections already written - Tone is still not sure why yet... need more discussion here
- Should consents be lumped in with education?
- Keith proposes to add a new section for education in either APH&P or APS profiles. Larry, Tone disagreed as this doesn't allow for reuse in other content profiles.
Clinical Questions
- (4/18 ts - from discussion with Mike Jolley) The top of Form E states "Plans/Education" - Which are plans? Which are education? This is important as it will help to determine how to code these data elements.
from Clinical T-Conn 5/1/08 (ts)
- This is an education list, and not a plan list. All plans should be listed in the APS document under Plan of Care
- It was proposed to add Tubal Sterilization Consent to this document as well as other consents (circumcision, etc.). I disagree with this and think it needs further discussion. Two other options were mentioned:
- Include with or near the Advanced Directives section in the APS document - this would be a change proposal
- Create a separate Antepartum Consent document (another profile) - I don't think we have time this year
- Mike Jolley will work on Snomed codes
UHIN Perinatal Data Elements
The link below contains a list of perinatal data elements identified as being important by UHIN, courtesy of Dr. Scott Williams of Hospital Corporation of America. media:UHIN Perinatal Data Elements.xls
The table below lists the data elements and maps them into the current work.
| Section Name Data Element Identifier | Sub-Section | Data element | Usage | Found in APR/APS |
Where? |
| Patient Demographics | |||||
| PD1 | Intake History Date Date the patient first encountered the office for the index pregnancy. |
Required Repeat 1 |
APR | serviceEvent/effectiveTime | |
| PD2 | Current Patient Name (Last, First, MI) - Name may change | Required Repeat n >=1 Please include all if there are more than one. |
APR | patient/name | |
| PD3 | Alias(s) Patient Name (Last, First, MI) - Name may change | Optional Repeat n >=1 |
APR | patient/name | |
| PD4 | Maiden patient name | Optional Repeat 1 |
APR | patient/name | |
| PD5 | Clinic medical record number Specify Site (free text) |
Optional Repeat n >1 |
APR | patientRole/id | |
| PD6 | Current Primary OB Provider Primary OB Provider (keep a history; associated with primary OB provider) |
Required Repeat n >=1 Please include all if there are more than one. |
APR | performer/assignedPerson/name | |
| Current Primary OB National Provider Identifier | APR | performer/id | |||
| PD7 | Current Primary OB Provider Group | Optional Repeat n >=1 |
APR | performer/representedOrganization | |
| Other Previous Prenatial Provider(s) with Dates | Optional Repeat n>=1 |
performer/time | |||
| PD8 | Newborn Physician | Optional Repeat n >=1 |
performer | ||
| PD9 | Referred By | Optional Repeat 1 |
performer | ||
| PD10 | Intended Facility For Delivery | Optional Repeat 1 |
|||
| PD11 | Hospital medical record number Specify Site (Free Text) |
Optional Repeat 1 |
|||
| PD12 | Master patient index number (may be organization specific now) | Optional Repeat 1 |
|||
| PD13 | Mothers Date of Birth | Required Repeat 1 |
patient/birthTime | ||
| PD14 | Father's Date of Birth (MO/Day/Yr) | Optional Repeat 1 |
|||
| PD15 | Mother of Baby Race | Optional Repeat n >=1 |
patient/raceCode | ||
| PD16 | Father of Baby -Race | Optional Repeat n >=1 |
See XPHR for FH | ||
| PD18 | Marital Status (S/M/W/D/SEP) Keep history |
Optional Repeat n >=1 |
patient/maritalStatus | ||
| PD19 | Mother of Baby- Occupation | Optional Repeat n >=1 |
See XPHR for FH | ||
| PD20 | Father of Baby- Occupation | Optional Repeat n >=1 |
See XPHR for FH | ||
| PD21 | Mother of Baby - Yrs of School | Optional Repeat 1 |
See XPHR for FH | ||
| PD22 | Father of Baby - Yrs of School | Optional Repeat 1 |
See XPHR for FH | ||
| PD23 | Mother of Baby Religion | Optional Repeat n >=1 |
patient/religiousPreferenceCode | ||
| PD24 | Father of Baby Religion | Optional Repeat n >=1 |
See XPHR for FH | ||
| PD25 | Mother's of Baby- Language | Optional Repeat n >=1 |
patient/languageCommunication | ||
| PD26 | Husband/Domestic Partner Name (Last, First, Mi) | Optional Repeat 1 |
participant/participantRole/associatedPerson/name | ||
| PD27 | Husband/Domestic Partner Phone | Optional Repeat n >=1 |
participant/participantRole/associatedPerson/name | ||
| PD28 | Father of Baby (Last, First) | Optional Repeat 1 |
participant/participantRole/associatedPerson/name | ||
| PD29 | Father of Baby Phone | Optional Repeat n >=1 |
participant/participantRole/associatedPerson/name | ||
| PD30 | Maternal GrandMother's Name | Optional Repeat 1 |
See XPHR for FH | ||
| PD31 | Maternal Grandmothers DOB | Optional Repeat 1 |
See XPHR for FH | ||
| PD32 | Maternal Grandfather's Name | Optional Repeat 1 |
See XPHR for FH | ||
| PD33 | Maternal Grandfather's DOB | Optional Repeat 1 |
See XPHR for FH | ||
| PD34 | Paternal Grandmother's Name | Optional Repeat 1 |
See XPHR for FH | ||
| PD35 | Paternal Grandmother's DOB | Optional Repeat 1 |
See XPHR for FH | ||
| PD36 | Paternal Grandfather's Name | Optional Repeat 1 |
See XPHR for FH | ||
| PD37 | Paternal Grandfaters DOB | Optional Repeat 1 |
See XPHR for FH | ||
| PD38 | Patient Living Address | Optional Repeat n >=1 |
patientRole/addr | ||
| PD39 | Patient Mailing Address | Optional Repeat n >=1 |
patientRole/addr | ||
| PD40 | Patient State | Optional Repeat n >=1 |
patientRole/addr/state | ||
| PD41 | Patient Zip | Optional Repeat n >=1 |
patientRole/addr/postalCode | ||
| PD42 | Residence of mother - Country | Optional Repeat n >=1 |
patientRole/addr/country | ||
| PD43 | Patient Home Phone | Optional Repeat n >=1 |
patientRole/telecom | ||
| PD44 | Patient Cell Phone | Optional Repeat n >=1 |
patientRole/telecom | ||
| PD45 | Patient Work Phone | Optional Repeat n >=1 |
patientRole/telecom | ||
| PD46 | Insurance Carrier Need a code for self-pay. Looping |
Optional Repeat n >=1 |
See XPHR for Payers | ||
| PD47 | Policy Holder Name | Optional Repeat n >=1 |
See XPHR for Payers | ||
| PD48 | Group Number | Optional Repeat n >=1 |
See XPHR for Payers | ||
| PD49 | Policy | Optional Repeat n >=1 |
See XPHR for Payers | ||
| PD50 | Emergency Contact Name | Optional Repeat n >=1 |
See XPHR for Contacts | ||
| PD51 | Emergency Contact Phone | Optional Repeat n >=1 |
See XPHR for Contacts | ||
| PD52 | "Did Mother get WIC food for herself" with the following qualifiers: Y, N, U | Optional Repeat n >=1 |
|||
| PERSONAL MEDICAL HISTORY | Send only positive responses - otherwise do not send All these should be in alphabetical order and include details for each disorder below in box |
||||
| PMH1 | Alcohol (amt/day pre preg; amt/day preg; years use, binge drinking (Y/N) freq) More than Y/N answer | Optional Repeat 1 |
|||
| PMH2 | Anesthesia Complications | Optional Repeat 1 |
See prior work on PPHP | ||
| PMH3 | Autoimmune Disorder | Optional Repeat 1 |
|||
| PMH4 | Breast Self Exam (yes or no) and freqency | Optional Repeat 1 |
|||
| PMH5 | Blood Disorder | Optional Repeat 1 |
|||
| PMH6 | Bladder Infections (1 or greater than 1) | Optional Repeat 1 |
|||
| PMH7 | Breast disease/surgery | Optional Repeat 1 |
|||
| PMH8 | Cancer/history of abnormal pap smear | Optional Repeat 1 |
|||
| PMH9 | Cancer History | Optional Repeat n >=1 |
|||
| PMH10 | Cardiac disease | Optional Repeat 1 |
|||
| PMH11 | Chemical or radiation exposure history Free Text 240 Characters |
Optional Repeat n >=1 |
|||
| PMH12 | Depression | Optional Repeat 1 |
|||
| PMH13 | Diabetes type 1 | Optional Repeat 1 |
|||
| PMH14 | Diabetes type 2 | Optional Repeat 1 |
|||
| PMH15 | Emotional and/or physical abuse | Optional Repeat 1 |
|||
| PMH16 | Gastrointestinal disease | Optional Repeat 1 |
|||
| PMH17 | GYN Surgery | Optional Repeat 1 |
|||
| PMH18 | History Blood transfusion | Optional Repeat 1 |
|||
| PMH19 | Infectious diseases | Optional Repeat 1 |
|||
| PMH20 | Illicit/recreational drugs (amt/day pre preg; amt/day preg; years use) More than Y/N answer | Optional Repeat 1 |
|||
| PMH21 | Infertility | Optional Repeat 1 |
|||
| PMH22 | History of Eating Disorder Dates |
Optional Repeat n >=1 |
|||
| PMH23 | Hypertension | Optional Repeat 1 |
|||
| PMH24 | Hypothyroid | Optional Repeat 1 |
|||
| PMH25 | Hyperthyroid | Optional Repeat 1 |
|||
| PMH26 | Kidney disease | Optional Repeat 1 |
|||
| PMH27 | Known uterine malformation | Optional Repeat 1 |
|||
| PMH28 | Liver disease | Optional Repeat 1 |
|||
| PMH29 | Neurologic/Seizure Disorder | Optional Repeat 1 |
|||
| PMH30 | Religious objections to medical treatment Text |
Optional Repeat 1 |
|||
| PMH31 | Special Diet Requirements Text |
Optional Repeat 1 |
|||
| PMH32 | Operations/hospitalizations (year & reason) | Optional Repeat 1 |
|||
| PMH33 | Other psychiatric problems | Optional Repeat 1 |
|||
| PMH34 | Organ transplant | Optional Repeat 1 |
|||
| PMH35 | Previous uterine surgery (excludes previous C-section) (check box for yes or no) | Optional Repeat 1 |
|||
| PMH36 | Pulmonary Disease Asthma | Optional Repeat 1 |
|||
| PMH37 | Pulmonary Disease other than Asthma | Optional Repeat n >=1 |
|||
| PMH38 | Stroke | Optional Repeat 1 |
|||
| PMH39 | STD - All | Optional Repeat 1 |
|||
| PMH40 | Thrombosis/varicosities/embolism/ phlebitis | Optional Repeat 1 |
|||
| PMH41 | Tobacco Use amt/day pre preg; amt/day 1st Trimester amt/day 2nd Trimester amt/day 3rd Trimester years use stop date:___ |
Optional Repeat 1 |
|||
| PMH42 | Thyroid disease | Optional Repeat 1 |
|||
| PMH43 | Unintentional injury | Optional Repeat 1 |
|||
| PMH44 | Other _______________ | Optional Repeat 1 |
|||
| INFECTION HISTORY | General Comment section for Infection History (also include a comments field) |
||||
| IH1 | Gential herpes | Optional Repeat 1 |
|||
| IH2 | Live with someone with TB or exposed to TB | Optional Repeat 1 |
|||
| IH3 | Other Infections:______________ | Optional Repeat 1 |
|||
| IH3 | Partner with genital herpes (Y) | Optional Repeat 1 |
|||
| IH4 | Rash or viral illness since last menstrual period (also include a comments field) |
Optional Repeat 1 |
|||
| ALLERGIES REACTIONS | General Comment section for Allergies/Reactions | ||||
| AR 1 | Drug allergies/reactions | Optional Repeat 1 |
APS | ||
| AR 2 | Food allergies | Optional Repeat 1 |
APS | ||
| AR 3 | Latex allergies/reactions | Optional Repeat 0 |
APS | ||
| AR 4 | Seasonal allergies | Optional Repeat 1 |
APS | ||
| AR 5 | Other allergies/reactions | Optional Repeat 1 |
APS | ||
| Medication History | Optional Repeat n >=1 |
||||
| MH1 | Medication Name This includes vitamins or herbs |
APS | |||
| MH2 | Dose | Optional Repeat 1 |
APS | ||
| MH3 | Start | Optional Repeat 1 |
APS | ||
| MN4 | Stop | Optional Repeat 1 |
APS | ||
| MH5 | Optional Repeat n >=1 |
Anti-D immune globulin (RhIG) given or date refused and 28 wks date (Result column has signature __________ blank line space) | Optional Repeat n>=1 |
||
| MH6 | MMR (date) | Optional Repeat n >=1 |
See XPHR for Immunizations | ||
| MH7 | Tetnus (date) | Optional Repeat n >=1 |
See XPHR for Immunizations | ||
| OBSTETRICAL HISTORY | FOR EACH PAST PREGNANCY | ||||
| OH1 | Pregnancy Order | Optional Repeat 1 |
APR | ||
| OH2 | Anesthesia Type: None Spinal Epidural General Local IV Sedation Other A,b,c,d,e for multiple births |
Optional Repeat n >=1 |
|||
| OH3 | Date Month/Year (none, epideral, general, narcotics, other ____ |
Optional Repeat 1 |
APR | ||
| OH4 | Delivery Type: vag operative vaginal c-section - Scar Type+F182 Separate fields for day, month and year |
Optional Repeat n >=1 |
|||
| OH5 | Birth Weight Pounds and Ounces Vaginial, c-section, vacuum, forceps (check all that apply) |
Optional Repeat 1 |
|||
| OH6 | GA Weeks | Optional Repeat 1 |
|||
| OH7 | Gender M/F/U | Optional Repeat 1 |
|||
| OH8 | Labor Length Units are hours | Optional Repeat 1 |
|||
| OH9 | Placed of Birth (Hospital, City/State) (Hours) |
Optional Repeat 1 |
|||
| OH10 | Pregnancy outcome: liveborn stillborn miscarriage abortion Ectopic |
Optional Repeat 1 |
|||
| OH11 | Still living (Y/N) If no death prior to 28 days. live, stillbirth, miscarriage, ectopic, |
Optional Repeat 1 |
|||
| OH12 | Previous cervical cerclage surgery | Optional Repeat n >=1 |
|||
| OH13 | How many months did it take you to achieve this pregnancy? (______months) (Please count the number of months in which intercourse occurred without using a contraceptive method. Also count months with any kind of medical treatment to get pregnant. If the pregnancy occurred while you were using a contraceptive method, answer 0.) | Optional Repeat n >=1 |
|||
| OH14 | Did you utilize infertility treatments to achieve this pregnancy? If yes, choose all that apply from the following options: oral ovulation induction drug - clomiphene citrate (Clomid, Serophene), letrazole (Femora), anastrazole (Arimidex) insulin sensitizing agent metformin (Glucophage), roziglitazone (Avandia), pioglitazone (Actos) an injectable fertility drug (gonadotropin) human menopausal gonadotropin (hMG), follicle stimulating hormone (FSH) human chorionic gonadotropin (hCG) to trigger ovulation or support your early pregnancy? progesterone supplementation (intramuscular [IM], vaginal, oral) during your attempt to become pregnant or during this pregnancy? artificial insemination In Vitro Fertilization (IVF) In Vitro Fertilization (IVF) with intracytoplasmic sperm injection (ICSI) Gamete Intrafallopian Transfer (GIFT) Zygote Intrafallopian Transfer (ZIFT) (You may choose as many treatments used specifically for this pregnancy. Do not include other treatments that occurred prior to this pregnancy.) |
Optional Repeat n >=1 |
|||
| COMPLICATION OF ANY PREGNANCY | Newborn problems - when known to have occurred in any pregnancy - include preganacy number | Include Pregnancy number and fetus number | |||
| CPN1 | Newborn Problems | Admit to NICU | Optional Repeat n >=1 |
||
| CPN2 | Newborn Problems | Anemia | Optional Repeat n >=1 |
||
| CPN3 | Newborn Problems | Anencephaly | Optional Repeat n >=1 |
||
| CPN4 | Newborn Problems | Asphyxia, in liveborn infant | Optional Repeat n >=1 |
||
| CPN5 | Newborn Problems | Aspiration - Meconium | Optional Repeat n >=1 |
||
| CPN6 | Newborn Problems | Aspiration - Other | Optional Repeat n >=1 |
||
| CPN7 | Newborn Problems | Birth Injury - Brachial Plexy Injury | Optional Repeat n >=1 |
||
| CPN8 | Newborn Problems | Birth Injury - Cephalhematoma | Optional Repeat n >=1 |
||
| CPN9 | Newborn Problems | Birth Injury - Other | Optional Repeat n >=1 |
||
| CPN10 | Newborn Problems | Cardiac defect | Optional Repeat n >=1 |
||
| CPN11 | Newborn Problems | Cerebral palsy | Optional Repeat n >=1 |
||
| CPN12 | Newborn Problems | Congenital abnormality | Optional Repeat n >=1 |
||
| CPN13 | Newborn Problems | Chromosomal abnormality | Optional Repeat n >=1 |
||
| CPN14 | Group B Strep | Optional Repeat 1 |
|||
| CPN15 | Newborn Problems | Hyperglycemia | Optional Repeat n >=1 |
||
| CPN16 | Newborn Problems | Hypoglycemia | Optional Repeat n >=1 |
||
| CPN17 | Newborn Problems | Hypovolemia | Optional Repeat n >=1 |
||
| CPN18 | Newborn Problems | Immune/alloimmune Thrombocytopenia | Optional Repeat n >=1 |
||
| CPN19 | Newborn Problems | Isoimmunization - ABO newborn | Optional Repeat n >=1 |
||
| CPN20 | Newborn Problems | Isoimmunization - Rh Newborn | Optional Repeat n >=1 |
||
| CPN21 | Newborn Problems | Isoimmunization - Other newborn | Optional Repeat n >=1 |
||
| CPN22 | Labor complications | IUGR - move to past preg newborn problems | Optional Repeat 1 |
||
| CPN23 | Newborn Problems | Jaundice | Optional Repeat n >=1 |
||
| CPN24 | Labor complications | Previous infant with GBS infection - move to past preg newborn problems | Optional Repeat n >=1 |
||
| CPN25 | Newborn Problems | Respiratory Distress Syndrome | Optional Repeat 1 |
||
| CPN26 | Newborn Problems | Sepis | Optional Repeat 1 |
||
| CPN27 | Newborn Problems | Thrombocytopenia | Optional Repeat 1 |
||
| CPN28 | Newborn Problems | Transitory Tachypnea of newborn | Optional Repeat 1 |
||
| CPN29 | Newborn Problems | Other newborn problems | Optional Repeat 1 |
||
| COMPLICATION OF ANY PREGNANCY | Fetal problems - when known to have occurred in any pregnancy - include preganacy number | ||||
| CPF1 | Anencephaly | Optional Repeat n >=1 |
|||
| CPF2 | Fetal demise | Optional Repeat 1 |
|||
| CPF3 | Fetal surgery | Optional Repeat 1 |
|||
| CPF4 | Cardiac defect | Optional Repeat n >=1 |
|||
| CPF5 | Congenital abnormality | Optional Repeat n >=1 |
|||
| CPF6 | Chromosomal abnormality | Optional Repeat n >=1 |
|||
| CPF7 | History of polyhydramnios - move to past preg newborn problems | Optional Repeat n >=1 |
|||
| CPF8 | History of oligohydramnios - move to past preg newborn problems | ||||
| CPF9 | IUGR - move to past preg newborn problems | Optional Repeat 1 |
|||
| CPF10 | Other fetal problems | Optional Repeat 1 |
|||
| CPF11 | Macrosomia | Optional Repeat 1 |
|||
| CPF12 | twin to twin transfusion | Optional Repeat 1 |
|||
| Maternal Complication of Past Pregnancies | Maternal Problems | Include when known to have occurred in any pregancy include pregancy number | |||
| MC1 | Maternal Problems | Bleeding requiring hospitalization Required transfusion |
Optional Repeat 1 |
||
| MC2 | Maternal Problems | Chorioamnionitis | Optional Repeat 1 |
||
| MC3 | Maternal Problems | DES exposure | Optional Repeat 1 |
||
| MC4 | Depression/Postpartum (check box for yes or no) | Optional Repeat 1 |
|||
| MC5 | Maternal Problems | Endometritis | Optional Repeat n >=1 |
||
| MC6 | Maternal Problems | GBS Carrier | Optional Repeat n >=1 |
||
| MC7 | Maternal Problems | Gestational Diabetes | Optional Repeat n >=1 |
||
| MC8 | Maternal Problems | Hyperemesis Gravidarum | Optional Repeat n >=1 |
||
| MC9 | Maternal Problems | Incompetent cervix | Optional Repeat n >=1 |
||
| MC10 | Maternal Problems | PROM (>+37 wks) | Optional Repeat 1 |
||
| MC11 | Maternal Problems | P-PROM (<37 wks) | Optional Repeat 1 |
||
| MC12 | Maternal Problems | Placenta Accreta | Optional Repeat 1 |
||
| MC13 | Maternal Problems | Placental Abruption - antepartum | Optional Repeat 1 |
||
| MC14 | Maternal Problems | Placenta previa | Optional Repeat 1 |
||
| MC15 | Maternal Problems | Postpartum hemorrhage Required transfusion |
Optional Repeat 1 |
||
| MC16 | Maternal Problems | Preeclampsia | Optional Repeat n >=1 |
||
| MC17 | HELLP Syndorme | Optional Repeat n >=2 |
|||
| MC18 | Maternal Problems | Preterm labor symptoms | Optional Repeat n >=1 |
||
| MC19 | Maternal Problems | Pulmonary embolism | Optional Repeat n >=1 |
||
| MC20 | Maternal Problems | Pyelonephritis | Optional Repeat n >=1 |
||
| MC21 | Maternal Problems | Trauma during pregnancy | Optional Repeat n >=1 |
||
| MC22 | Maternal Problems | Urinary Tract infection | Optional Repeat n >=1 |
||
| MC23 | Maternal Problems | Uterine atony | Optional Repeat n >=1 |
||
| MC24 | Maternal Problems | Uterine Inversion | Optional Repeat n >=1 |
||
| MC25 | Maternal Problems | Vaginal infection | Optional Repeat n >=1 |
||
| MC26 | Maternal Problems | Other maternal problems | Optional Repeat n >=1 |
||
| Labor complications of any past pregnancy | Labor complications | Include when known to have occurred in any pregancy include pregancy number |
|||
| LC1 | Labor complications | Amniotic fluid embolism | Optional Repeat n >=1 |
||
| LC2 | Labor complications | Cord prolapse | Optional Repeat n >=1 |
||
| LC3 | Labor complications | Elevated maternal temperature | Optional Repeat n >=1 |
||
| LC4 | Labor complications | Failed forceps delivery | Optional Repeat n >=1 |
||
| LC5 | Labor complications | Failed vacuum delivery | Optional Repeat n >=1 |
||
| LC6 | Labor complications | Inadvertant Cystomy | Optional Repeat n >=1 |
||
| LC7 | Labor complications | Labor Dystocia (failure to progress) | Optional Repeat n >=1 |
||
| LC8 | Labor complications | Non- reassuring fetal heart rate | Optional Repeat n >=1 |
||
| LC9 | Labor complications | Placental Abruption intrapartum | Optional Repeat n >=1 |
||
| LC10 | Labor complications | Post-partum hemorrhage | Optional Repeat n >=1 |
||
| LC11 | Labor complications | Precipitous delivery | Optional Repeat n >=1 |
||
| LC12 | Labor complications | Shoulder dystocia | Optional Repeat 1 |
||
| LC13 | Labor complications | Uterine Rupture | Optional Repeat 1 |
||
| LC14 | Labor complications | Vasa Previa | Optional Repeat 1 |
||
| LC15 | Labor complications | 4th degree Vaginal laceration | Optional Repeat n >=1 |
||
| LC16 | Labor complications | Other labor complications | Optional Repeat n >=1 |
||
| RISK FACTORS | For preterm birth (also include a comments field) |
Other risk factors need to be pulleed in here for presentation | |||
| RFP1 | 2 or more abortions requiring D & C | Optional Repeat 1 |
|||
| RFP2 | Labor complications | Age less than 18 or greater than 35 | Optional Repeat 1 |
||
| RFP3 | Labor complications | Black race | Optional Repeat 1 |
||
| RFP4 | Labor complications | Cervical insufficiency | Optional Repeat 1 |
||
| RFP5 | History of STDs | Optional Repeat 1 |
|||
| RFP6 | Prior preterm birth (less than 37 weeks) | Optional Repeat 1 |
|||
| RFP7 | Weight less than 120 pounds | Optional Repeat 1 |
|||
| RISK FACTORS | For general adverse pregnancy Outcomes | Need to pull items from other sections for presentation | |||
| RFG1 | Labor complications | Infertility greater than one year | |||
| RFG2 | Labor complications | Infertility: Asst. Rep. Technology | |||
| RFG3 | Labor complications | Morbid Obesity Also include a comments field |
|||
| RFG4 | Labor complications | Other Risk Factors:_______________ | Optional Repeat n >=1 |
||
| Menstrual History | |||||
| MNH1 | Menarche (Age onset) | Optional Repeat 1 |
|||
| MNH2 | Menses Regular (Y/N); | Optional Repeat 1 |
|||
| MNH3 | Usual Duration of the Cycle (days) | Optional Repeat 1 |
|||
| MNH4 | Usual Duration of the Bleeding (days) | Optional Repeat 1 |
|||
| Gestational Age Determinants | |||||
| GAD1 | LMP | Last Menstrual Period Date Definite Approximate Unknown |
Optional Repeat 1 |
||
| GAD2 | Normal amount/duration of LMP (Y/N) | Optional Repeat 1 |
|||
| GAD3 | Hormonal contraceptive at conception (Y/N) | Optional Repeat 1 |
|||
| GAD4 | Estimated gestational age by LMP | Optional Repeat 1 |
|||
| GAD5 | Estimated due date by LMP | Optional Repeat n >1 |
|||
| GAD6 | PG Test Positive (Date) | Optional Repeat 1 |
|||
| GAD7 | 1st Visit | Optional Repeat 1 |
|||
| GAD8 | Date of Ultrasound | Optional Repeat n >=1 |
|||
| GAD9 | Estimated gestational age by ultrasound | Optional Repeat n >=1 |
|||
| GAD10 | Estimated due date by ultrasound | Optional Repeat n >=1 |
|||
| GAD11 | gestational age calculated field based on EDD |
||||
| GAD12 | Quickening - date | ||||
| GAD13 | fundal height at umbilicus - date | ||||
| GAD14 | Final EDD (Date) Current | Optional Repeat n >=1 |
|||
| GAD15 | Final EDD Method based on Options listed LMP, Ultrasound, Positive PG test, Quickening (Fetal Movement) |
Optional Repeat n >=1 |
|||
| GAD16 | Date of Last Revision | Optional Repeat n >=1 |
|||
| Genetic/Teratology Screening | Check box throughout for Patient and baby's father and any family members from either mother or father - send if known to be present radiation exposure in 1st trimester Also include a comments field for each field below |
||||
| GTS1 | Prescription drugs, supplements, vitamins, herbs, OTC drugs)/illicit/recreational drugs/alcohol since last menstrual period List all |
Optional Repeat n >=1 |
|||
| GTS2 | Family Hx of birth defects | Optional Repeat n >=1 |
|||
| GTS3 | Tay sachs (check if positive or abnormal) | Optional Repeat n >=1 |
|||
| GTS4 | Sickle cell trait/disease (check if positive or abnormal) | Optional Repeat n >=1 |
|||
| GTS5 | Thalassemia (check if positive or abnormal) | Optional Repeat n >=1 |
|||
| GTS6 | Huntington chorea | Optional Repeat n >=1 |
|||
| GTS7 | Cystic Fibrosis | Optional Repeat n >=1 |
|||
| GTS8 | Muscular Dystrophy | Optional Repeat n >=1 |
|||
| GTS9 | Hemophilia or other blood disorders | Optional Repeat n >=1 |
|||
| GTS10 | Neural tube defect (meningomyelocele, spina bifida, or anencephaly) | Optional Repeat n >=1 |
|||
| GTS11 | Down syndrome | Optional Repeat n >=1 |
|||
| GTS12 | Hydrocephaly | Optional Repeat n >=1 |
|||
| GTS13 | Congenital heart defect | Optional Repeat n >=1 |
|||
| GTS14 | Is there a family hisotry Mental retardation/autism | Optional Repeat n >=1 |
|||
| GTS15 | Is there a f+E313amily history of fragile X? | Optional Repeat n >=1 |
|||
| GTS16 | Other inherited genetic or chromosomal disorder (check yes or no) metabolic disorder (eg, type 1 diabetes, pku) (check yes or no) |
Optional Repeat n >=1 |
|||
| GTS17 | Maternal metabolic disorder (eg, type 1 diabetes, pku) | Optional Repeat n >=1 |
|||
| GTS18 | Any other Please list: | Optional Repeat n >=1 |
|||
| GTS19 | Canavan disease | ||||
| GTS20 | Familial Dysautonomia chicken pox or immunization (yes or no) |
||||
| GTS21 | Maternal history of chicken pox during this pregnancy | Optional Repeat n >=1 |
|||
| GTS | DES exposure (yes or no) | Optional Repeat 1 |
|||
| GTS | PKU (yes/ no ) Mother | Optional Repeat n >=1 |
|||
| GTS | DES exposure (yes or no) | Optional Repeat 1 |
|||
| GTS | PKU (yes/ no ) Other Child | Optional Repeat n >=0 |
|||
| Physical Examination | Send all elements with value of Normal = N Abnormal = A Not Performed = NP |
Optional Repeat n>=1 |
|||
| PE1 | Additional physical Exam Date | Optional Repeat n >=1 |
|||
| PE2 | Mother's Height | ||||
| PE3 | Mother's current weight" | ||||
| PE4 | Mother's Prepregnancy weight | Optional Repeat 1 |
|||
| PE5 | BP ____, Temp ____ | Optional Repeat n >=1 |
APS | Flowsheet | |
| PE6 | HEENT (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE7 | BREASTS (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE8 | LUNGS (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE9 | HEART (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE10 | ABDOMEN (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE11 | EXTREMITIES (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE12 | SKIN (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE13 | LYMPH NODES (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE14 | Rectum (check box for normal or abnormal) Allow Text for abnormal result |
Optional Repeat 1 |
APR | Physical Exam | |
| PE15 | Other physical findings: | Optional Repeat n >=1 |
APR | Physical Exam | |
| PE16 | Examiner's Signature ____________ | Optional Repeat 1 |
|||
| PE17 | Pelvic Exam | Pelvic exam date | Optional Repeat n>=1 |
||
| PE18 | VULVA Normal Abnormal or Not Done List Abnormalities |
Optional Repeat 1 |
|||
| PE19 | VAGINA Normal Abnormal or Not Done List Abnormalities |
Optional Repeat 1 |
|||
| PE20 | CERVIX Normal Abnormal or Not Done List Abnormalities |
Optional Repeat 1 |
|||
| PE21 | UTERUS Size (____ Weeks | Optional Repeat 1 |
|||
| PE22 | UTERUS Normal Abnormal or Not Done List Abnormalities |
Optional Repeat 1 |
|||
| PE23 | ADNEXA Normal Abnormal or Not Done List Abnormalities |
Optional Repeat 1 |
|||
| PE24 | Pelvic Dimensions (Adequate, Borderline, Contracted) | Optional Repeat 1 |
|||
| PE25 | Diagonal Conjugate Reached, Not Reached or ________CM | Optional Repeat 1 |
|||
| PE26 | Spines (check box for Average, prominent or blunt) List Abnormalities |
Optional Repeat 1 |
|||
| PE27 | Sacrum (check box for concave, straight or anterior) List Abnormalities |
Optional Repeat 1 |
|||
| PE28 | Subpubic Arch (check box for normal,wide, or narrow) List Abnormalities |
Optional Repeat 1 |
|||
| PE29 | Gynecoid Pelvic Type Gynecoid Anthropoid Android Platypoid |
Optional Repeat 1 |
|||
| PE30 | Other physical findings: | Optional Repeat n >=1 |
|||
| PE31 | Pain Scale Scale 1-10 |
Optional Repeat 1 |
|||
| PE32 | Examiner's Name | Optional Repeat 1 |
|||
| PE33 | National Provider Identifier | Optional Repeat 2 |
|||
| Prenatal Examinations | |||||
| PNE1 | 45 available rows columns include: weeks gest (best est), fundal height (CM), presentation, FHR, fetal movement, Cervix exam (dil./eff. Sta.) ultrasound cervical length, blood pressure (2 fields) , weight, next appointment date (mm/dd/yy) heart rate, fetal movement, contractions comments Separate all elements |
Optional Repeat n>=1 |
APS | Flowsheet | |
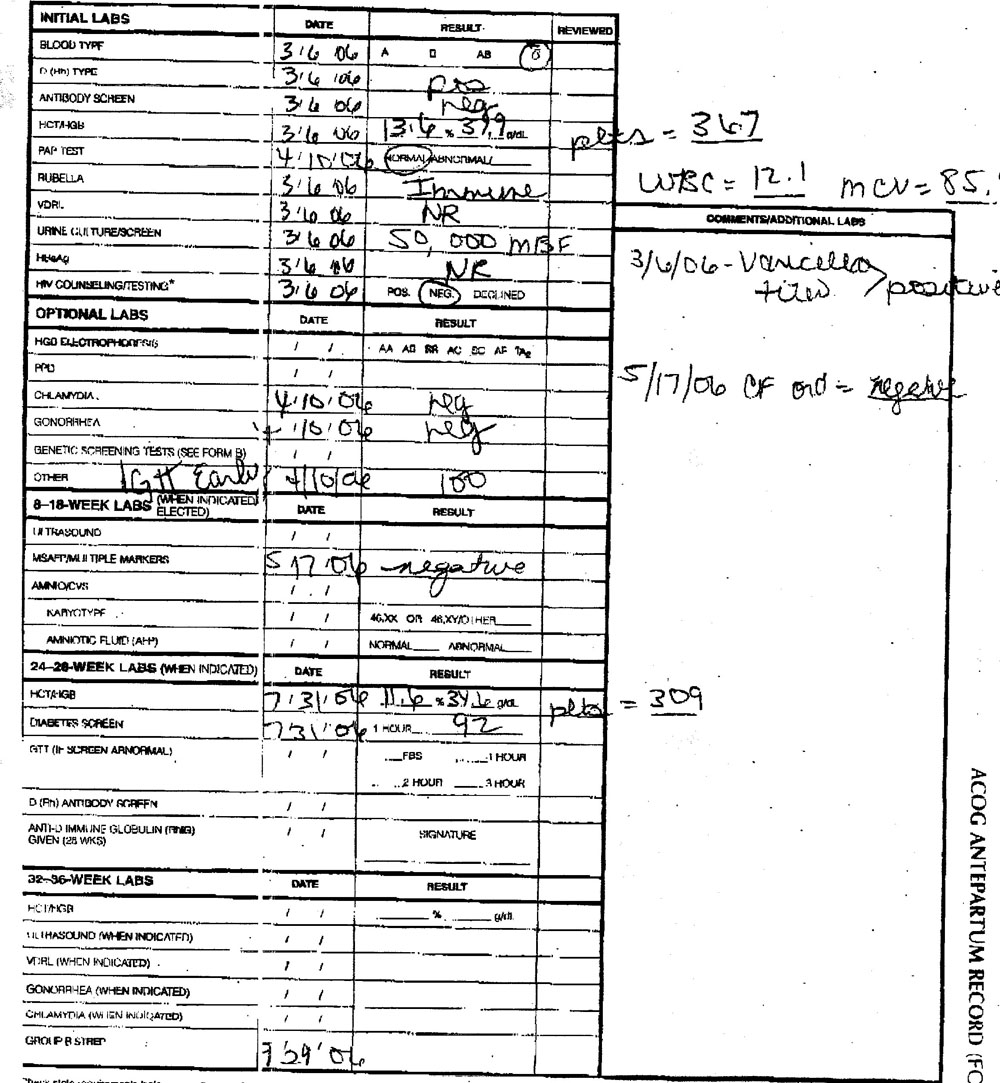
| Laboratory | |||||
| L1 | Blood type, (Patient) A B AB O | Optional Repeat 1 |
APR | ||
| L2 | Blood type, (Father of the baby, if known) A B AB O | Optional Repeat 1 |
|||
| L3 | D (Rh) Type (patient) | Optional Repeat 1 |
APR | ||
| L4 | D (Rh) Type (Father of the baby, if known) | Optional Repeat 1 |
|||
| L5 | 2 sections for Antibody Screen (check box for pos, neg and space for the titer) | Optional Repeat n >=1 |
|||
| L6 | beta-hCG | Optional Repeat n >=1 |
|||
| L7 | HGB, (Result)___g/dl | Optional Repeat n >=1 |
|||
| L8 | HCT (Result) ___% | Optional Repeat n >=1 |
|||
| L9 | Pap Test, (Result) Normal/abnormal/__ | Optional Repeat n >=1 |
|||
| L10 | Rubella (check box for IMM, N-Imm and _______(blank space)). | Optional Repeat n >=1 |
|||
| L11 | VDRL | Optional Repeat n >=1 |
|||
| L12 | RPR | Optional Repeat n >=1 |
|||
| L13 | Urinalysis | Optional Repeat n >=1 |
|||
| L14 | Urine Culture (check box for pos, neg and __________(blank space)) | Optional Repeat n >=1 |
|||
| L15 | Hepatitis B s AG | Optional Repeat n >=1 |
|||
| L16 | HIV Counsel/Testing, (Result) POS NEG Declined (***Check state requirements before recording results**) | Optional Repeat 1 |
|||
| L17 | HIV Counseling | Optional Repeat 1 |
|||
| L17 | HIV (check box for Offer/Date | Optional Repeat 1 |
|||
| L18 | HIV Decline/Date | Optional Repeat 1 |
|||
| L18 | Chlamydia | Optional Repeat n >=1 |
|||
| L19 | Gonorrhea | Optional Repeat n >=1 |
|||
| L20 | Aneuploidy screening | Optional Repeat n >=1 |
|||
| L21 | HGB Electrophoresis, (Result) AA AS SS AC SC AF A2 | Optional Repeat n >=1 |
|||
| L22 | PPD | Optional Repeat n >=1 |
|||
| L23 | Genetic Screening Tests | Optional Repeat n >=1 |
|||
| L24 | First Trimester Screeingin with nuchal translucency and maternal serum. (Check box for normal, abnormal?) | Optional Repeat n >=1 |
|||
| L25 | Other | Optional Repeat n >=1 |
|||
| L26 | Ultrasound | Optional Repeat n >=1 |
|||
| L27 | Amnios | Optional Repeat n >=1 |
|||
| L28 | MSAFP/Multiple Markers | Optional Repeat n >=1 |
|||
| L29 | Chorionic villus sampling | Optional Repeat n >=1 |
|||
| L30 | Karyotype ____________ (blank line space) | Optional Repeat n >=1 |
|||
| L31 | Amniotic Fluid (AFP) Include Value and Reference Range | Optional Repeat n >=1 |
|||
| L32 | Individual columns for: 24-28-week labs, date (common throughout), result (common throughout), reviewed (common throughout); | ||||
| L33 | Maternal Serum Quad Screen (check box for Offer, Decline, Abn and NL) | Optional Repeat n >=1 |
|||
| L34 | Maternal Serum Triple Screen (check box for Offer, Decline, Abn and NL) | Optional Repeat n >=1 |
|||
| L35 | Diabetes Screen (Result column has 1 hour __________(blank line space)) space for High end cutoff value |
Optional Repeat n >=1 |
|||
| L36 | GTT (if screen abnormal) (Result column has ___FBS, ___1 hour, ___ 2 hour, ___ 3 hour) | Optional Repeat n >=1 |
|||
| L37 | Strep Type B A G C F |
Optional Repeat n >=1 |
|||
| L38 | TSH __________(blank space) | Optional Repeat n >=1 |
|||
| L39 | Thryoid Free T3 Free T4 |
||||
| L40 | VZV Ab (check box Pos and Neg) | Optional Repeat 1 |
|||
| L41 | CF Counseling/Screening (check box for Offer, Decline, Pos and Neg) | Optional Repeat 1 |
|||
| L42 | Comments/additional Labs blank space section | Optional Repeat n >=1 |
|||
| L43 | Influenza vaccine provided If yes - date and dose |
Optional Repeat n>=1 |
|||
consider adding back:
Physical Exam
- Adnexa || ||SNOMED CT ||R || ||BL || ||normal
abnormal - Diagonal Conjugate || ||SNOMED CT ||O || ||CD || ||reached
not reached
length - Spines ||163576005 ||SNOMED CT ||O || ||CD || ||average
prominent
blunt - Sacrum ||164565001 ||SNOMED CT ||O || ||CD || ||concave
straight
anterior - Subpubic Arch || ||SNOMED CT ||O || ||CD || ||normal
wide
narrow - Gynecoid Pelvic Type ||163555000 ||SNOMED CT ||O || ||BL || ||yes
no - Cervix ||309668003 ||SNOMED CT ||R || ||BL || ||normal
abnormal - Uterus Size ||163509002(fundus = term size)
163498004(gravid uterus size) ||SNOMED CT ||R ||weeks gestation, fibroids determined from ultrasound ||BL || || - All values SHALL have a normal/abnormal (BL) value and a text narrative with related comments. The elements with value sets other than normal/abnormal (e.g. vulva, vagina) have value sets that may change and therefore should not be coded to a specific value set.
- |Funduscopic Examination || ||LOINC ||O || || || ||