ACWP State of the Art: Difference between revisions
| Line 2: | Line 2: | ||
== State of the Art == | == State of the Art == | ||
Access Control is about controlling who may access what data for what purpose. The general idea is to provide healthcare providers with the information they need to know – and no more. The underlying rules are usually derived from medical workflows, legal regulations (e. g. privcy legislative), patient consents, and security regulations within a healthcare organization. These rules are explicitely or implicitly bound to conditions that state when and how a rule is to be applied. Sets of related rules and conditions are called policies. | |||
Policies might be implicit in a way that every node within a distributed system is configured to behave compliant with certain rules that all partners have agreed upon. Especially in situations where access control rules are influenced by authorities that are independent from the enforcing nodes (e. g. patient privacy consents) or where rules are rather complex and context-aware (e. g. access rights for nurses, dietary staff, and other non-physicians) a policy language can be used to express a policy in a machine-interpretable manner. Examples for such languages are given in section 6 of this white paper. | |||
In this section the state-of-the-art with respect to policy controlled access management is sketched. Especially three of the most important aspects will be discussed in more detail: | |||
* what rules of thumb have to be considered when designing policies and an architecture for their management and enforcement | |||
* what policy paradigms are relevant with respect to typical access control problems in healthcare | |||
* what core building blocks can be found with any access control solution | |||
===Principles of Secure Design=== | ===Principles of Secure Design=== | ||
* '''Economy of Mechanism:''' The used mechanism must be kept as simple as possible. It should also target a well-confined issue instead of trying to cover each and every eventuality. | * '''Economy of Mechanism:''' The used mechanism must be kept as simple as possible. It should also target a well-confined issue instead of trying to cover each and every eventuality. With respect to access control in healthcare one should always consider whether technically driven access control, organizational rules, or reactive measures - e. g. logging - are most appropriate for the implementation of different access restrictions. | ||
* '''Complete Mediation:''' Every access attempt must be explicitly safe-guarded through the access management mechanisms at all times. This also implies that there must be no possibility to avoid the access management (even for special roles/functions such as administrators) while accessing any resource. | * '''Complete Mediation:''' Every access attempt must be explicitly safe-guarded through the access management mechanisms at all times. This also implies that there must be no possibility to avoid the access management (even for special roles/functions such as administrators) while accessing any resource. For healthcare systems complete mediation is rarely given because the most common way to deal with emergency situations is to bypass the whole access control subsystem. For a secure design a solution should be defined where an emergency context just activates a specific policy that can be decided upon using the same mechanisms as any other policy. | ||
* '''Open Design:''' All algorithms and security mechanisms have to be openly available and fully check- and verifiable. | * '''Open Design:''' All algorithms and security mechanisms have to be openly available and fully check- and verifiable. | ||
* '''Least-Common Mechanism:''' Mechanisms, system states and objects, which are capable of explicitly or implicitly granting access rights, should not be shared between different users and/or applications. For each individual user or application, a different mechanism or an instantiation of the same mechanism should be used. | * '''Least-Common Mechanism:''' Mechanisms, system states and objects, which are capable of explicitly or implicitly granting access rights, should not be shared between different users and/or applications. For each individual user or application, a different mechanism or an instantiation of the same mechanism should be used. | ||
* '''Fail-Safe Defaults:''' Addresses the principle that anything which is not allowed | * '''Fail-Safe Defaults:''' Addresses the principle that anything which is not explicitly allowed is denied by default. That means in practice, that any access attempt, which may not be explicitly and entirely verified as allowed, is automatically denied. Privileges are admitted exclusively to an initially empty set of rights (opt-in in favour of opt-out rules). | ||
* '''Separation of Privilege:''' | * '''Separation of Privilege:''' Whenevver possible, security and safe-guarding mechanisms should ensure that multiple conditions, which exist independently from each other, are fully checked and validated before granting any rights. Policies should be defined in a way that a subject must match multiple attributes before access is granted to sensitive patient data (e. g. a user must match a certain role and issue the request from a trusted system). | ||
* '''Least Privileges:''' Any identity should only be granted with the least set of access rights possible in order to complete its assigned function or task. If any right needs to be added to perform extraordinary duties, the right may be granted when actually required and discarded after the completion of the non-standard task. | * '''Least Privileges:''' Any identity should only be granted with the least set of access rights possible in order to complete its assigned function or task. If any right needs to be added to perform extraordinary duties, the right may be granted when actually required and discarded after the completion of the non-standard task. | ||
* '''Psychological Acceptability:''' Mechanisms securing and safe-guarding access to a resource may not add unnecessary complexity to the user or complicate the user to execute the granted right of accessing that resource unjustifiably. | * '''Psychological Acceptability:''' Mechanisms securing and safe-guarding access to a resource may not add unnecessary complexity to the user or complicate the user to execute the granted right of accessing that resource unjustifiably. Missing psychological acceptance usually leads to situations where users find creative ways to bypass many of the other design principles (e. g. everyone in a hospital department uses the most priviledged account). | ||
* '''Reluctance to Trust:''' External systems, individuals, users, and objects should be always considered as insecure. A certain level of trust in external elements may only be granted, when explicitly supported by adequate security certifications, such as Common Criteria [CC 3.1]. Furthermore, it is imperative to limit and minimise the amount of mechanisms, systems, and objects, which are to be fully trusted required for the access control/management. | * '''Reluctance to Trust:''' External systems, individuals, users, and objects should be always considered as insecure. A certain level of trust in external elements may only be granted, when explicitly supported by adequate security certifications, such as Common Criteria [CC 3.1]. Furthermore, it is imperative to limit and minimise the amount of mechanisms, systems, and objects, which are to be fully trusted required for the access control/management. | ||
* '''Privacy Consideration:''' Any identity should only have access to exactly that fraction or portion of the data, which is immediately required in order to fulfil its current task in its current role/function. | * '''Privacy Consideration:''' Any identity should only have access to exactly that fraction or portion of the data, which is immediately required in order to fulfil its current task in its current role/function. | ||
* '''Isolation:''' All access control/management mechanisms should be isolated from other systems, operated independently, and must be specially secured. | * '''Isolation:''' All access control/management mechanisms should be isolated from other systems, operated independently, and must be specially secured. | ||
| Line 31: | Line 40: | ||
* Mandatory Access Control (MAC): The validation and grant of access rights is performed by utilising sensitivity levels/labels, rules, and/or policies. In the simplest case (multi-level) sensitivity each object and each user posses a set of security attributes: the user is usually assigned a clearance level, whereas the resource is assigned to a sensitivity level. Rules determine how those levels may concretely correlate and whether and how users of one clearance level may grant access rights to other users of different clearance levels. The MAC-style access control model - with a certain degree of tweaks and modifications - is implemented and utilised in most of the operating systems. | * Mandatory Access Control (MAC): The validation and grant of access rights is performed by utilising sensitivity levels/labels, rules, and/or policies. In the simplest case (multi-level) sensitivity each object and each user posses a set of security attributes: the user is usually assigned a clearance level, whereas the resource is assigned to a sensitivity level. Rules determine how those levels may concretely correlate and whether and how users of one clearance level may grant access rights to other users of different clearance levels. The MAC-style access control model - with a certain degree of tweaks and modifications - is implemented and utilised in most of the operating systems. | ||
* Role-Based Access Control (RBAC): The RBAC-model is not assigning access rights to any resource directly to a subject's identity. Instead, each subject's identity is assigned with a set of roles, in which any access rights are defined. The concrete executing of access rights is therefore not directly bound to the user but acquired through its current role. The roles and its concrete permissions may be defined hierarchical (hierarchical RBAC) and rules may be constructed, which defines limitations (constraints) for the role assignment and permissions-granting (constrained RBAC). | * Role-Based Access Control (RBAC): The RBAC-model is not assigning access rights to any resource directly to a subject's identity. Instead, each subject's identity is assigned with a set of roles, in which any access rights are defined. The concrete executing of access rights is therefore not directly bound to the user but acquired through its current role. The roles and its concrete permissions may be defined hierarchical (hierarchical RBAC) and rules may be constructed, which defines limitations (constraints) for the role assignment and permissions-granting (constrained RBAC). | ||
* Most countries' laws constitute the patient as the souvereign of his medical data (''my body - my data - my control''). Therefore the patient implicitetly is the owner of his data and the only one to grant access permissions. This leads to a DAC influence on every access control solution in healthcare. This influence is rather implicit in an intra-enterprise scenario where a treatment contract is usually signed by the patient which transfers part of the patient's rights to the hospital (which is as well part of the DAC paradigm). In an inter-enterprise or cross-domain scenario this DAC-portion of the access policy is much more visible and usually expressed by a patient privacy consent. | |||
===Policy Based Access Control (PEP, PDP, ...)=== | ===Policy Based Access Control (PEP, PDP, ...)=== | ||
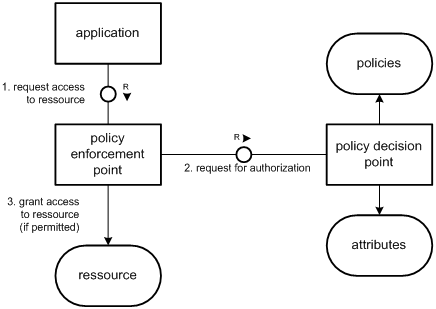
All commercial implementations of the above named and described access control models are based upon the strict separation - as illustrated in figure | All commercial implementations of the above named and described access control models are based upon the strict separation - as illustrated in the figure below - of the Policy Enforcement and Policy Decision [RFC 2753, RFC 3198, ISO-10181-3]: | ||
* A policy is considered to be a set of rules, which are controlling the security- and privacy-behaviour of a given system. The security policies addressed in this paper are defining, what subjects may - under what constraints with what operations - access what objects. | * A policy is considered to be a set of rules, which are controlling the security- and privacy-behaviour of a given system. The security policies addressed in this paper are defining, what subjects may - under what constraints with what operations - access what objects. | ||
* A Policy Enforcement Point (PEP) intercepts all access attempts for any resources safe-guarded by the access control/management and forwards those requests to the PDP. Afterwards it receives the policy decision of the PDP and enforces its result against the requester. | * A Policy Enforcement Point (PEP) intercepts all access attempts for any resources safe-guarded by the access control/management and forwards those requests to the PDP. Afterwards it receives the policy decision of the PDP and enforces its result against the requester. | ||
Revision as of 18:13, 19 January 2009
IHE White Paper on Access Control
State of the Art
Access Control is about controlling who may access what data for what purpose. The general idea is to provide healthcare providers with the information they need to know – and no more. The underlying rules are usually derived from medical workflows, legal regulations (e. g. privcy legislative), patient consents, and security regulations within a healthcare organization. These rules are explicitely or implicitly bound to conditions that state when and how a rule is to be applied. Sets of related rules and conditions are called policies.
Policies might be implicit in a way that every node within a distributed system is configured to behave compliant with certain rules that all partners have agreed upon. Especially in situations where access control rules are influenced by authorities that are independent from the enforcing nodes (e. g. patient privacy consents) or where rules are rather complex and context-aware (e. g. access rights for nurses, dietary staff, and other non-physicians) a policy language can be used to express a policy in a machine-interpretable manner. Examples for such languages are given in section 6 of this white paper.
In this section the state-of-the-art with respect to policy controlled access management is sketched. Especially three of the most important aspects will be discussed in more detail:
- what rules of thumb have to be considered when designing policies and an architecture for their management and enforcement
- what policy paradigms are relevant with respect to typical access control problems in healthcare
- what core building blocks can be found with any access control solution
Principles of Secure Design
- Economy of Mechanism: The used mechanism must be kept as simple as possible. It should also target a well-confined issue instead of trying to cover each and every eventuality. With respect to access control in healthcare one should always consider whether technically driven access control, organizational rules, or reactive measures - e. g. logging - are most appropriate for the implementation of different access restrictions.
- Complete Mediation: Every access attempt must be explicitly safe-guarded through the access management mechanisms at all times. This also implies that there must be no possibility to avoid the access management (even for special roles/functions such as administrators) while accessing any resource. For healthcare systems complete mediation is rarely given because the most common way to deal with emergency situations is to bypass the whole access control subsystem. For a secure design a solution should be defined where an emergency context just activates a specific policy that can be decided upon using the same mechanisms as any other policy.
- Open Design: All algorithms and security mechanisms have to be openly available and fully check- and verifiable.
- Least-Common Mechanism: Mechanisms, system states and objects, which are capable of explicitly or implicitly granting access rights, should not be shared between different users and/or applications. For each individual user or application, a different mechanism or an instantiation of the same mechanism should be used.
- Fail-Safe Defaults: Addresses the principle that anything which is not explicitly allowed is denied by default. That means in practice, that any access attempt, which may not be explicitly and entirely verified as allowed, is automatically denied. Privileges are admitted exclusively to an initially empty set of rights (opt-in in favour of opt-out rules).
- Separation of Privilege: Whenevver possible, security and safe-guarding mechanisms should ensure that multiple conditions, which exist independently from each other, are fully checked and validated before granting any rights. Policies should be defined in a way that a subject must match multiple attributes before access is granted to sensitive patient data (e. g. a user must match a certain role and issue the request from a trusted system).
- Least Privileges: Any identity should only be granted with the least set of access rights possible in order to complete its assigned function or task. If any right needs to be added to perform extraordinary duties, the right may be granted when actually required and discarded after the completion of the non-standard task.
- Psychological Acceptability: Mechanisms securing and safe-guarding access to a resource may not add unnecessary complexity to the user or complicate the user to execute the granted right of accessing that resource unjustifiably. Missing psychological acceptance usually leads to situations where users find creative ways to bypass many of the other design principles (e. g. everyone in a hospital department uses the most priviledged account).
- Reluctance to Trust: External systems, individuals, users, and objects should be always considered as insecure. A certain level of trust in external elements may only be granted, when explicitly supported by adequate security certifications, such as Common Criteria [CC 3.1]. Furthermore, it is imperative to limit and minimise the amount of mechanisms, systems, and objects, which are to be fully trusted required for the access control/management.
- Privacy Consideration: Any identity should only have access to exactly that fraction or portion of the data, which is immediately required in order to fulfil its current task in its current role/function.
- Isolation: All access control/management mechanisms should be isolated from other systems, operated independently, and must be specially secured.
References:
- Saltzer, J. H.; Schroeder, M. D.: The Protection of Information in Computer Systems. Proceedings of the ACM. Vol. 63, Nr. 9. pp. 1278-1308. 1975.
- Wallach, Dan; Balfanz, Dirk; Dean, Drew; Felten, Edward: Extensible Security Architectures for Java. In: Proc. 16th Symposium on Operating Systems Principles, October 1997, Saint-Malo, France. [[1]]
- Benantar, Messaoud (Ed.): Access Control Systems. Springer. 2006.
- Bishop, Matt. Computer Security: Art and Science. Boston, MA: Addison-Wesley, 2003
- Ferraiolo, David; Kuhn, Richard; Chandramouli, Ramaswamy: Role-Based Access Control. Artech House. 2. Auflage, 2007.
- Build Security In. Website of the US Department of Homeland Security.[[2]]
Access Control Paradigms: DAC, MAC, RBAC, ...
The three fundamental access control paradigms, which may be found and distinguished in practice today, are:
- Discretionary Access Control (DAC): the validation and grant of access permissions is solely performed on the basis of the concrete identity of a subjects and its group membership. Subjects who possess access rights for a certain resource may pass those on to other subjects. In a quite common implementation of DAC (such as used in UNIX), to each resource a special property called the "owner" is assigned, who may exclusively grant or deny any access rights to users or other groups for this resource. However, in a typical DAC-style model, it may not be avoidable that a user may acquire access rights for resources - through the means mentioned above - which this user should not posses conventionally.
- Mandatory Access Control (MAC): The validation and grant of access rights is performed by utilising sensitivity levels/labels, rules, and/or policies. In the simplest case (multi-level) sensitivity each object and each user posses a set of security attributes: the user is usually assigned a clearance level, whereas the resource is assigned to a sensitivity level. Rules determine how those levels may concretely correlate and whether and how users of one clearance level may grant access rights to other users of different clearance levels. The MAC-style access control model - with a certain degree of tweaks and modifications - is implemented and utilised in most of the operating systems.
- Role-Based Access Control (RBAC): The RBAC-model is not assigning access rights to any resource directly to a subject's identity. Instead, each subject's identity is assigned with a set of roles, in which any access rights are defined. The concrete executing of access rights is therefore not directly bound to the user but acquired through its current role. The roles and its concrete permissions may be defined hierarchical (hierarchical RBAC) and rules may be constructed, which defines limitations (constraints) for the role assignment and permissions-granting (constrained RBAC).
- Most countries' laws constitute the patient as the souvereign of his medical data (my body - my data - my control). Therefore the patient implicitetly is the owner of his data and the only one to grant access permissions. This leads to a DAC influence on every access control solution in healthcare. This influence is rather implicit in an intra-enterprise scenario where a treatment contract is usually signed by the patient which transfers part of the patient's rights to the hospital (which is as well part of the DAC paradigm). In an inter-enterprise or cross-domain scenario this DAC-portion of the access policy is much more visible and usually expressed by a patient privacy consent.
Policy Based Access Control (PEP, PDP, ...)
All commercial implementations of the above named and described access control models are based upon the strict separation - as illustrated in the figure below - of the Policy Enforcement and Policy Decision [RFC 2753, RFC 3198, ISO-10181-3]:
- A policy is considered to be a set of rules, which are controlling the security- and privacy-behaviour of a given system. The security policies addressed in this paper are defining, what subjects may - under what constraints with what operations - access what objects.
- A Policy Enforcement Point (PEP) intercepts all access attempts for any resources safe-guarded by the access control/management and forwards those requests to the PDP. Afterwards it receives the policy decision of the PDP and enforces its result against the requester.
- A Policy Decision Point (PDP) may decide on the concrete outcome of an incoming authorisation request. In order to do that, the PDP is applying the best-fitting policy and may determine additional security attributes when necessary. Then the PDP is executing the policy onto the incoming authorisation request. The result - coded in form of a policy decision - defines whether the requested access operation is granted or denied.

XACML [XACML 1.0] defines two further actors:
- The Policy Adiminstration Point (PAP) who is basically administering and keeping the policies.
- The Policy Information Point (PIP) which facilitates the PDP to acquire any additional security attributes of resources and subjects in order to determine whether an access request is to be granted or denied.
Standards (SAML, WS*, XACML, XSPA, ...)
Author's Note: Standards are discussed in detail in Standards and Specs to be considered in chapter 6.
Discussion
place issues to be discussed among the editorial team here...
Change Requests
place your change requests here...