Difference between revisions of "Nursing Use Cases"
Jump to navigation
Jump to search

m (New page: Three use cases developed to explore the Functional Status Assessment Integration Profile are described in futher detail below. # [[#Long-Term Care to Acute Care|Long-Ter...) |
m (→Behavioral) |
||
| (2 intermediate revisions by the same user not shown) | |||
| Line 7: | Line 7: | ||
{{Note|Italicized text in the use cases below denote information in the use case that provides details regarding patient condition and workflow, but will not be included as part of the content integration profile.}} | {{Note|Italicized text in the use cases below denote information in the use case that provides details regarding patient condition and workflow, but will not be included as part of the content integration profile.}} | ||
| − | ==Long-Term Care to Acute Care== | + | ==<span id='uc1'>Long-Term Care to Acute Care</span>== |
[[Image:FSA1.png|center|480px|Long-Term Care to Acute Care Process Flow]] | [[Image:FSA1.png|center|480px|Long-Term Care to Acute Care Process Flow]] | ||
| Line 48: | Line 48: | ||
## Patient returns to LTC. | ## Patient returns to LTC. | ||
| − | ==Home or Ambulatory Care into Acute Care == | + | ==<span id='uc2'>Home or Ambulatory Care into Acute Care</span> == |
[[Image:FSA2.png|center|480px|Home or Ambulatory Care into Acute Care Process Flow]] | [[Image:FSA2.png|center|480px|Home or Ambulatory Care into Acute Care Process Flow]] | ||
; Primary Actor(s): ED Nurse, ED Doctor, Surgeon, Orthopedic nurse in acute care facility, Nurse in rehab facility, Clinical staff in assisted living facility | ; Primary Actor(s): ED Nurse, ED Doctor, Surgeon, Orthopedic nurse in acute care facility, Nurse in rehab facility, Clinical staff in assisted living facility | ||
| Line 106: | Line 106: | ||
## Patient's assisted living needs have been updated to reflect fall risk and assistance with ambulation, toileting and transfer in the electronic health record. | ## Patient's assisted living needs have been updated to reflect fall risk and assistance with ambulation, toileting and transfer in the electronic health record. | ||
| − | ==Behavioral== | + | ==<span id='uc3'>Behavioral</span>== |
[[Image:FSA3.png|center|480px|Behavioral Process Flow]] | [[Image:FSA3.png|center|480px|Behavioral Process Flow]] | ||
Latest revision as of 15:12, 2 August 2007
Three use cases developed to explore the Functional Status Assessment Integration Profile are described in futher detail below.
- Long-Term Care to Acute Care - describes a use case for assessment information during transfers of care from long term to acute care.
- Home or Ambulatory Care into Acute Care - describes a use case for assessment information during multiple care transfers.
- Behavioral - describes a use case for assessment information during transfers of care where information about depression in an older patient is used.
| Note: | Italicized text in the use cases below denote information in the use case that provides details regarding patient condition and workflow, but will not be included as part of the content integration profile. |
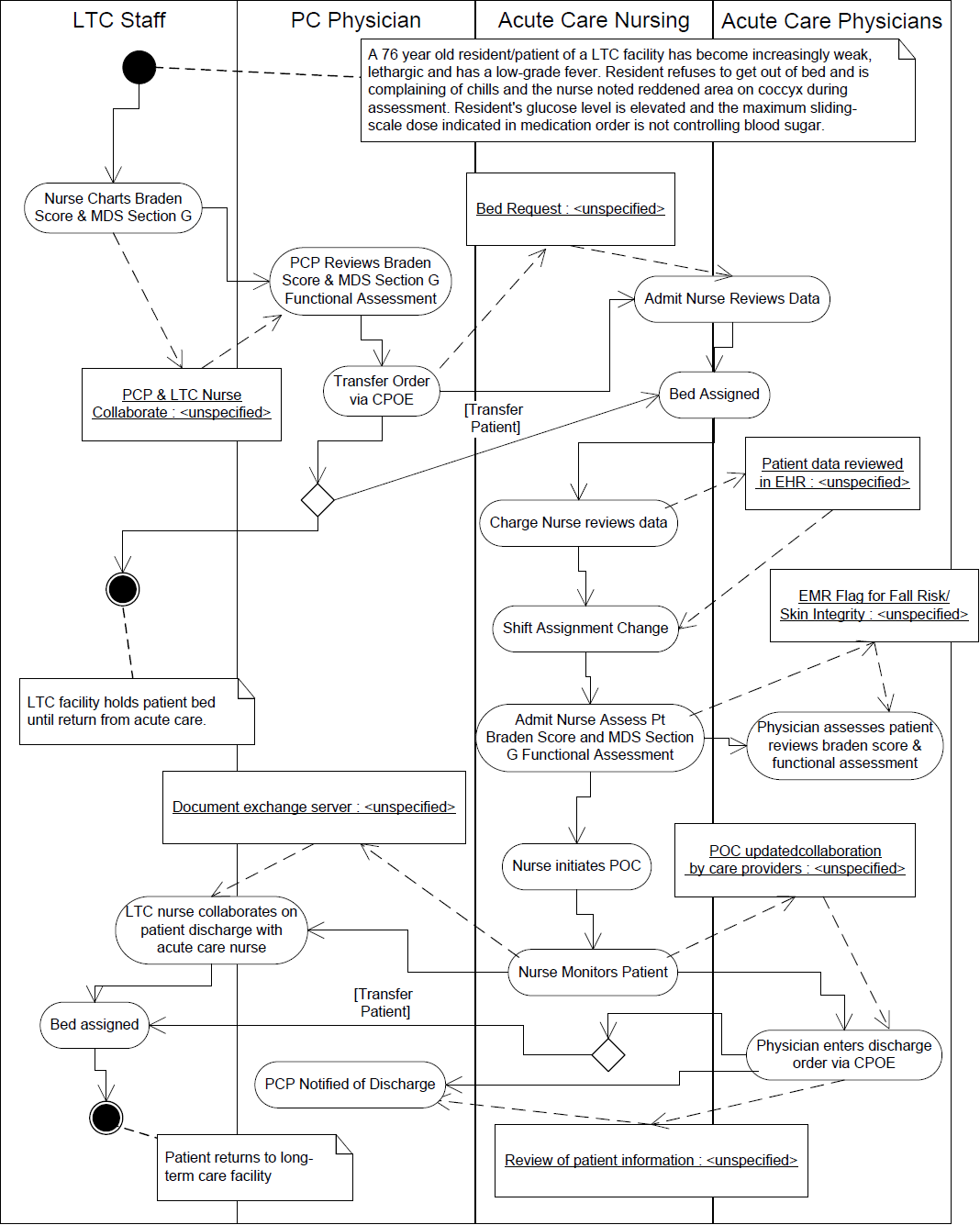
Long-Term Care to Acute Care

- Primary Actor(s): Discharge nurse in LTC facility, Admitting nurse in acute care facility
- Stakeholder(s): Primary Care Physician, Hospitalist
- Use Case Overview: A diabetic nursing home patient is transferring from the LTC environment to an in-patient acute care hospital based on deteriorating functional status assessments.
- Use Case Scenario
- A 76 year old resident/patient of a LTC facility has become increasingly weak, lethargic and has a low-grade fever. Resident refuses to get out of bed and is complaining of chills and the nurse noted reddened area on coccyx during assessment. Resident's glucose level is elevated and the maximum sliding-scale dose indicated in medication order is not controlling blood sugar.
- Nurse documents vital signs.
- Nurse documents finger-stick glucose measurement.
- Nurse documents current functional assessment.
- Nurse documents braden score.
- Nurse initiates phone collaboration with Primary Care Provider (PCP).
- Primary care provider(PCP)and nurse review patient status information on the electronic health record (EHR). Note: Interdisciplinary collaboration supports evaluation of physiologic changes and critical thinking leading to early intervention.
- PCP enters transfer order to acute care facililty via computerized physician order entry (CPOE).
- The patient's baseline and serial functional assessment data is sent to the acute care hospital via a document exchange server.
- Nurse admission coordinator reviews transfer documents via the EHR. Note: Early comprehensive patient information availability allows the admission coordinator to assign appropriate unit and adjust staffing based on potential acuity. Appropriate nurse to patient acuity staffing ratios support both staff and patient safety, reducing risk of errors.
- Bed is assigned on medical floor at acute care facility, pending admission is sent to charge nurse on the medical floor.
- Charge nurse reviews the patient's functional status assessment data, VS, glucose values and braden score from LTC facility. Note: The charge nurse is provided additional time to reassign other patients and/or allowing the admitting nurse more time to prepare for the patient admission.
- Based on the information reviewed, Charge nurse adjusts shift assignment based on patients level of care.
- Patient arrival to medical floor at acute care facility.
- Admitting nurse takes patient VS and completes admission assessment in EHR. Note: Nurse compares serial EHR preadmission assessments to new admission assessment data. Serial EHR assessments allow nurse to compare baseline assessement to last assessment at LTC and first hospital assessment supporting critical thinking related to discharge goals.
- Nurse records admission assessment data in EHR and EHR identifies pressure sore risk due to Braden Score total and fall risk.
- Electronic health record flags need for skin care protocol to clinician. Note: Electronic notifications are an adjunct to support the critical thinking skills of the nurse taking care of the patient and reinforce the proactive monitoring and management of patient's safety needs.
- An individualized patient plan of care (POC) initiated by nurse in EHR.
- Skin care protocol and fall risk protocol implemented according to facility protocols.
- Acute care physician assesses patient and reviews serial preadmission and current nurse assessment data in EHR. Physician adds to plan of care. Note: Having one location (EHR) for documentation from all disciplines saves time by reducing time needed to find various documentation paper tools. One EHR also supports communication and collaboration between clinicians, minimizing potential for errors.
- Patient's medical issues are addressed during course of hospitalization (5 days).
- Patient's individualized POC is reviewed and updated daily by each clinician. Note: Clinician is able to review data on-line and quickly update based on availability of previous data. Plan of care and prior knowledge of baseline allow relevent and reachable goals for discharge.
- Progress and level of care requirement is continuously monitored by nurse and hospitalist assigned to patient
- After several days of care, patient ready for discharge as evidenced by blood sugar levels WNL and increased functional status (including ambulation with assistance).
- Series of functional assessments and overal progress reviewed by care providers.
- Patient POC goals met, except level of functional status and unresolved skin risk as noted in EHR.
- Acute care physician enters discharge order via CPOE.
- PCP notified of transfer back to LTC facility and review of patient statusincluding unresolved issues.
- Long Term Care/Hospital collaborate on discharge plan/transfer. Note: Multiple series of assessment and POC data can be quickly reviewed and compared to maximize safety in transfer and supports interdisciplinary decision making to reach patient goals.
- Patient readied for discharge, EHR documents completed.
- EHR discharge documents sent to document exchange server; message sent to LTC to download documents.
- Patient returns to LTC.
Home or Ambulatory Care into Acute Care

- Primary Actor(s)
- ED Nurse, ED Doctor, Surgeon, Orthopedic nurse in acute care facility, Nurse in rehab facility, Clinical staff in assisted living facility
- Secondary Actor(s)
- Paramedics, Physical Therapist
- Stakeholder(s)
- Primary Care Physician, Hospitalist
- Use Case Overview
- A normally active, older adult in an assisted living community has an accidental fall requiring admission to an acute care facility. Alteration in functional status requires the patient discharge to a nursing home for rehabilitation with the long term goal of returning to assisted living.
- Use Case Scenario
- A 69 year old single male, living in an assisted community, is normally very active and self sufficient and requires only minimal assistance from staff for medication management. While walking outside, the patient falls, right lower extremity alignment changes noted. The patient has a large 10 cm hematoma on his side with bruising that extends down his right hip and leg. A laceration on his forehead noted, possibly from his glasses breaking during the fall. The patient is pale, and complaining of severe pain in his right hip. The patient is unable to move and an ambulance is called. Patient is transferred from the assisted living community to the emergency department at an acute care facility. There is no baseline functional assessment data available from the assisted living community. Medical information is maintained on EHR in assisted living.
- Nurse charts vital signs
- Nurse documents information regarding hematoma, area of bruising on right side and notes alignment changes.
- Nurse documents information regarding head laceration and covers wound with 2x2 gauze/tape.
- Primary care physician is notified of ambulance transfer to acute care facililty
- The patient's history from the assisted living community is reviewed with the paramedics before the patient is moved to the ambulance prior to transfer to the acute care facility emergency department.
- Paramedics are provided with a brief summary of patient including age, date of birth, medical history, medications and allergies.
- Patient is brought to emergency department of acute care facility and is assessed by clinical staff. Nurse and physician assigned to patient review accident information and patient history via the electronic health record. The nurse performs a thorough assessment of the patient's current condition, x-rays and labs are ordered. Patient is medicated for pain prior to the x-ray.
- ED nurse charts vital signs and accident information in electronic health record.
- ED nurse assesses patient's level of pain using numeric rating scale in the electronic health record.
- ED nurse notifies doctor of pain score.
- ED doctor assesses patient and reviews history.
- ED doctor orders hip x-ray and pain medication in electronic health record. ED doctor determines patient has hip fracture and recommends patient be transferred to the orthopedic floor with a surgical consult.
- ED doctor writes up admission to ortho floor and orders surgical consult in the electronic health record.
- Patient transferred to orthopedic floor at acute care facility and has surgical consult.
- Admitting nurse takes patient VS and completes admission assessment including numeric rating scale for pain and Braden scale for pressure risk in the electronic health record.
- The electronic health record evaluates admission assessment data entered by the clinician and flags patient for skin integrity problem and fall risk.
- Skin care and fall risk protocol implemented in the electronic health record according to facility protocols.
- Nurse documents numeric response to pain medication.
- Surgeon assesses patient condition and recommends total hip replacement surgery.
- Patient has surgery and returns to orthopedic floor. Nurses continue to monitor patient, provide interventions and assess pain level and medicate as needed. Patient begins physical therapy 1st day post-op.
- Individualized patient plan of care initiated in electronic health record.
- Patient's individualized POC is reviewed and updated daily by each clinician. Note: Clinician is able to review data on-line and quickly update based on availability of previous data. Plan of care and prior knowledge of baseline allow relevent and reachable goals for discharge.
- Patient's pain level is assessed pre and post medication using numeric rating scale and documented in electronic health record.
- Progress and level of care requirement is continuously monitored by nurse, surgeon and physical therapist assigned to patient.
- Physical therapist establishes rehabilitation plan and goals post total hip surgery and documents progress in electronic health record, adding rehabilitation goals to POC. Note: Interdisciplinary care planning and documentation on single EHR minimizes time spent documenting by eliminating repetition and redundancy while focusing on patient goals. Patient focus by interdisciplinary team reduces length of stay.
- Individualized patient plan of care initiated in electronic health record.
- Patient regains strength and is able to transfer and toilet with assistance. Staples have been removed from hip incision and bruising is resolving. Patients level of pain has dropped significantly since admission and is requiring less pain medication.
- Skin care protocol is suspended.
- Patient plan of care updated to reflect level of care patient requires.
- After several days of care post total hip surgery, the patient is progressing, but still not able to function independently (at previous baseline). The surgeon recommends the patient be transferred to a rehabilitation facility for more intense therapy.
- Series of functional assessments and overal progress reviewed by interdisciplinary team.
- Plan of care is updated in the electronic health record.
- Primary care physician is notified of plan to transfer.
- Patient is prepared for discharge to rehabilitation facility with final assessment completed.
- The patient's baseline and recent functional status assessments are sent to the rehabilitation facility via a document exchange server.
- Rehabilitation facility nurse admission coordinator reviews transfer documents.
- Bed is assigned on orthopedic floor at rehabilitation facility.
- Notification of pending admission is sent to charge nurse on the floor at the rehabilitation facility.
- Charge nurse reviews patient accident history, functional assessment data, and patient progress from acute care facility. Based on the information reviewed, nurse determines that patient will require assistance transferring, toileting and ambulation and will be at risk for falls.
- Rehab facility charge nurse adjusts shift assignment based on patients level of care. # Patient regains strength and is able to transfer, toilet and ambulate with minimal assistance after one week and has not required pain medicine the last 3 days. Surgeon recommends patient for transfer back to assisted living facility.
- Series of functional assessments and overal progress reviewed by care providers.
- Plan of care is updated in EMR system.
- Primary care physician is notified of plan to transfer patient back to assisted living facility.
- Patient is prepared for discharge to assisted living facility with final assessment completed.
- The patient's baseline and recent functional status assessments are sent to the assisted living facility via a document exchange server. Note: Early transfer of health information and plan of care facilitates maximum planning for safety and patient's arrival.
- Series of functional assessments and overal progress from rehabilitation center is reviewed by assisted living care providers.
- Assisted living clinical staff review patients hospitalization and rehab history, functional assessment data, and patient progress. Based on the information reviewed, nurse determines that patient will require assistance transferring, toileting and ambulation and will be at risk for falls.
- Series of functional assessments and overal progress reviewed by interdisciplinary care team.
- Patient's assisted living needs have been updated to reflect fall risk and assistance with ambulation, toileting and transfer in the electronic health record.
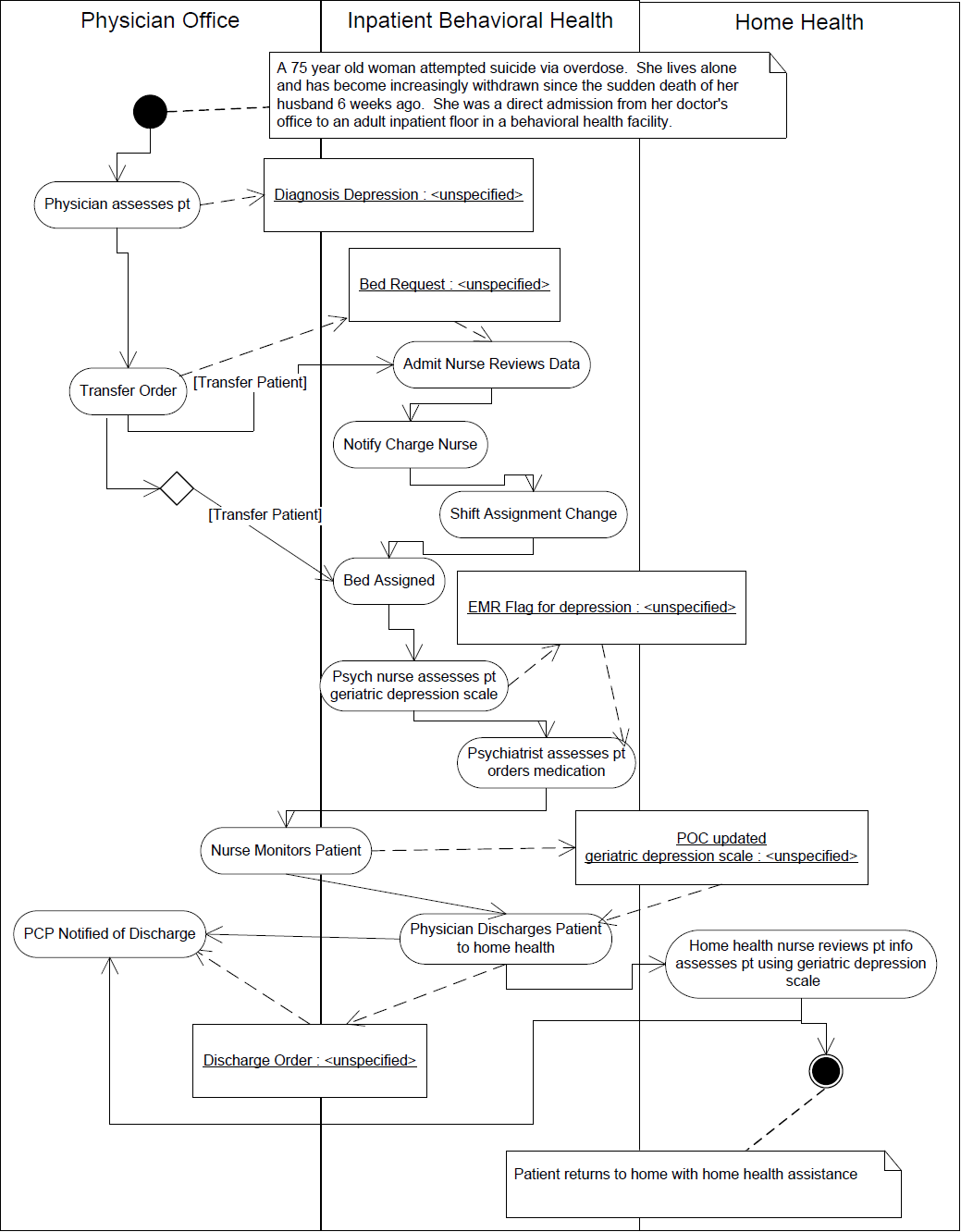
Behavioral

- Primary Actor(s)
- Psychiatric nurse, Attending physician/hospitalist, Home health nurse
- Stakeholder(s)
- Primary Care Physician, Outpatient psychiatrist
- Use Case Overview
- A recently widowed 75 year old woman is admitted to an adult inpatient floor of a behavior health hospital for depression post suicide attempt
- Use Case Overview
- A 75 year old woman who lives alone and has become increasingly withdrawn since the sudden death of her husband 6 weeks ago took several days worth of medication at one time from her pill pack. A neighbor found the confused elderly woman in the woman's home, and immediately took her to her psychiatrists office. Patient was diagnosed as depressed by her psychiatrist, and was a direct admission from her doctor's office to an adult inpatient floor in a behavioral health facility.
- Psychiatrist notes patient issue regarding depression into electonic health record notes.
- Patient screened by adult inpatient admission nurse using the geriatric depression scale. Her initial score was 26, indicating severe depression. Patient information was entered into the electronic health record. Patient states that she has a hard time getting going each day and is afraid of how she will survive without her husband. She has lost her appetite and is unhappy with her life without her husband.
- Nurse documents geriatric depression scale results in the electronic health record.
- Nurse documents patient's feelings and concerns in progress notes in the electronic health record.
- Nurse initiates plan of care for management of depression.
- Psychiatrist reviews the patient's progress and visits patient. Psychiatrist orders anti-depressant and mood stabilizer medications via CPOE.
- Social work evaluates the patient for her social support and financial status. The patient has no limitations in activity of daily living. She has a housekeeper come in monthly to clean and does her own grocery shopping and laundry weekly. Her nearest relative is over 1,000 miles away and her only support network are friends and neighbors that are also frail and elderly. The social worker also collaborates with the nurse regarding the signs of depression and the geriatric depression scale score. The plan of care is updated by the social worker and discharge planning begins.
- Daily, nursing gives patient medication and assesses the patient's depression status using the geriatric depression scale. Interventional therapy sessions provided to patient to improve mood and outlook for the future.
- Nurse documents administration of medication.
- Nurse documents depression assessment.
- Nurse documents patient's response to therapies.
- Nurse documents udpate to the plan of care.
- After 5 days, patient is progressing well and responding to therapy. Most recent geriatric depression scale score documented in the electronic health record is 15, indicating mild depression.
- Nurse documents administration of medication.
- Nurse documents depression assessment.
- Nurse documents patient's response to therapies.
- Plan of care updated by nurse and social worker.
- Patient care conference is done with patient, nurse, social worker and physician. Based on progress, patient will be discharged to home with home health visits.
- Patient's plan of care is updated and unresolved issues to be managed by home health services.
- Physician enters discharge to home order with home health services into the electronic health record.
- Patient is discharged home with home health referral.
- Home health nurse reviews patient status electronically and prepares for visit to patient home.
- Home health nurse reviews geriatric depression scale ratings from hospital and history of patient stay and underlying issues. Note: Communication of needs and depression status support early intervention by home health staff, minimizing length of time in care.
- Home health nurse visits patient at home.
- Nurse assesses patient using the geriatric depression scale and enters into the electronic health record.
- Nurse assesses patient using oasis and enters into the electronic health record.
- Outpatient psychiatrist reviews patient's progress from home health and follows up with patient. Note: Availability of EHR documentation to all providers of care to this patient supports continuity of care.
- Psychiatrist reviews continuing progress of geriatric depression scale rating since in electronic health record.
- Psychiatrist reviews home health Oasis assessment information in electronic health record.
- Outpatient psychatric appointment made by home health nurse for continuity of care. Note: Interoperable patient information available to provider at the point of care reduces redundant provision of care, thereby reducing cost, but protects patient safety during the transitions.